- Men
- Bilateral Scrotal Orchidectomy
- Bladder Neck Incision (B.N.I.) and Urethrotomy
- Brachytherapy
- Circumcision
- Cystoscopy
- Flexible Cystoscopy
- Hydrocelectomy Spermatocelectomy & Epididymal Cystectomy
- Inguinal Orchidectomy
- Kidney Cryotherapy
- Laparoscopic Nephrectomy
- Laproscopic Pyeloplasty
- Laser Prostatectomy
- Magnetic Resonance Imaging (MRI) Scan
- Nephrectomy
- Orchidopexy
- Other Services (Men & Women)
- Other Treatments (Men Only)
- Robotic Assisted Laparoscopic Prostatectomy
- Sexual Dysfunction
- Transperineal Ultrasound Guided Prostate Biopsy (TPPB)
- Transrectal Ultrasound & Biopsies of the Prostate
- Transurethral Resection of Bladder Tumour
- Ureteroscopy
- Vasectomy
- Women
- Children
- Clinical Trials
Treatment Process:
Nephrectomy
This information is designed to help you, your family and friends prepare for your surgery. It will also help you plan how to take care of yourself in the weeks following discharge from hospital.
A nephrectomy is an operation to remove one of the two bean-shaped kidneys that sit at the back of the abdominal cavity. The kidneys make urine by filtering waste products and excess fluid from the blood. Urine drains from the kidneys, through the ureters into the bladder where it is stored until the person is ready to go to the toilet.
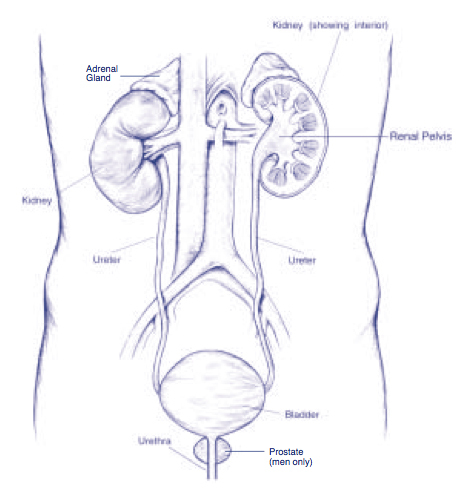
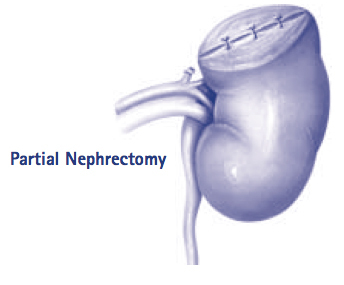
A nephrectomy involves removing an entire kidney through an incision in the flank, the side of the body between the ribs and the hip. In a small number of cases if a person has poor kidney function or if they only have one kidney, a partial nephrectomy may be done which means only part of the kidney is removed.
A nephrectomy is usually done for one of two reasons, either for cancer of the kidney or because of a non-functioning kidney.
- In the case of kidney cancer a radical nephrectomy is done. A radical nephrectomy is done in an attempt to rid the body of cancer by removing the entire kidney, adrenal gland, protective shell with its surrounding fat and attached vessels. In more advanced cases it may be done to stop continued bleeding from the effected kidney.
- For non-functioning kidneys, which are either caused by large stones, a lack of blood supply or abnormal kidney structure, a simple nephrectomy is done. With a simple nephrectomy only the kidney itself it taken from within its protective shell and the adrenal gland and other structures are left behind. A simple nephrectomy is usually done to avoid recurrent infection and the possibility of severe illness because of infection.
Treatment
As mentioned above the operation is usually done through a flank incision. However, in a small number of cases when cancer is suspected, depending on where the tumour is, a higher or lower incision may be needed or an incision in the abdomen may be necessary.
After the incision has been made, the blood supply to the kidney is isolated and tied off and the kidney is removed either with or without its surrounding structures. The wound is then closed with staples, or a dissolving stitch that dissolves slowly in the months following surgery. A wound drain may be inserted to drain any wound ooze. This is usually stitched in place and stays in for 2 days. A catheter (drainage tube which drains urine from the bladder) is also put in to monitor the urine output from the remaining kidney. The catheter usually stays in for 1-2 days, or until you are up and about. If you have had a partial nephrectomy, you may have a stent which is a plastic tube that runs from the kidney to the bladder. This helps the kidney to heal. It will be removed under local anaesthetic in the outpatients department about 4 – 6 weeks after your surgery.
Nephrectomy is a relatively common operation that takes approximately 2-3 hours to perform and involves a hospital stay of around 3 – 4 nights.
Your Consent
We need your permission for your operation to go ahead. Before you sign the consent form, it is important that you understand the risks and effects of the operation and anaesthetic. Your doctor and the nurse will discuss this with you, should you have any questions, your nurse or doctor would be happy to answer these.
There is a chance with this operation that you will need a blood transfusion. However, if you do need a blood transfusion and you want to refuse one, it is vital that you tell your surgeon and nurse prior to your operation. It is sometimes possible to donate some of your own blood prior to surgery. If you would like to do this, please discuss it with your surgeon.
If you would like your kidney returned to you for personal reasons, please discuss this with your family and inform your nurse and surgeon before your operation.
About Your Anaesthetic
You will NOT be allowed to eat or drink anything for at least six hours before your surgery. This includes chewing gum and sweets.
This type of surgery requires a general anaesthetic, which means you will be asleep throughout the operation and remember nothing of it. This may be used in combination with an Epidural, where a solution is injected into your back that will numb the lower half of your body.
After your surgery if you do not have an epidural anaesthetic, you may have a P.C.A pump attached to the drip in your arm. P.C.A stands for Patient Controlled Analgesia. It is a computer-controlled machine that delivers pain relief through your drip. You will be able to control the amount of pain relief given but the anaesthetist prescribes the maximum dose. You will receive more information about the P.C.A. pump and your anaesthetic at the pre-assessment clinic.
Feel free to discuss these options and any questions with the anaesthetist.
Your Operation
On admission, you will be informed of an approximate operation time and prepared for theatre by your nurse.
You may be fitted with T.E.D. stockings that help aid circulation and prevent blood clots, which there is always a slight risk of with surgery. You may also be instructed about special deep breathing and leg exercises that you should do after surgery.
A shave of the surgical site is required. This is usually done just prior to going to theatre or in theatre itself once you are asleep.
You may be given some tablets before theatre. These are charted by your anaesthetist and may include tablets for tension, nausea and pain prevention.
You will be escorted to the theatre, where you will be transferred to the theatre table. Anaesthetic staff will then insert a drip in your arm and will attach various monitoring devices. Once you have been completely prepared and given your anaesthetic, surgery will begin.
When the operation is completed, you will go to the recovery room where you will be cared for until you are ready to be transferred to the ward.
After Surgery
Your nurse will check your blood pressure and pulse regularly. Your wound and the drainage from it will also be monitored closely.
You will have a drip in your arm to make sure you receive adequate fluids. This will be removed once you are drinking normally. You can usually drink after surgery, depending on what was done during surgery. You may eat once you are tolerating fluids. You may have a P.C.A. pump connected to your drip or you will be kept comfortable by an epidural infusion, which numbs the lower half of the body.
Your urine will drain from your bladder, through the catheter into a bag. Your nurse will measure your urine output every hour. The urine is likely to be blood stained; this usually clears within the first 24 hours. The catheter is held inside your bladder by a small, inflated balloon, which prevents it from slipping out.
Day one after your operation
The morning after surgery the nurse will help you get up into a chair for a wash by the bedside or if you feel up to it you can go for a shower.
You will be told if you can eat and drink. Until you are able to drink, your drip will keep you well hydrated and provide the nutrients you need. You will usually also be given intravenous antibiotics through the drip to prevent any infection.
You will be given regular pain relievers, such as Panadol to help keep you comfortable. You should do regular deep breathing and leg exercises after surgery until you are fully mobile. The physiotherapist may come and see you to give further instructions.
Day two or three after your operation
If the drainage from your wound drain is minimal, it will be removed. Your catheter will also be removed when you are mobile and your urine output is sufficient.
You will be helped to walk down for a shower and at this time, your wound dressing is usually removed.
If you are comfortable enough on regular oral pain relievers, you will have your P.C.A. or epidural removed. The drip is not completely removed until the course of post-operative antibiotic treatment is complete. The need for antibiotics and the length of treatment will be different in each individual case but usually last about two to three days.
Usually by the second day after surgery for a simple nephrectomy, and by the third day for a radical nephrectomy, all the drains and tubes have been removed. All the sutures used are dissolving so do not need to be removed, however if wound staples are used these usually stay in for 7 to 10 days and are taken out by your own doctor or by the district nurse.
Going Home
You will be given a discharge letter that contains helpful information about how to care for yourself when you get home.
Your nurse will inform you about taking mild pain relievers, should you have any pain or discomfort after you return home.
You will be given or sent an outpatient appointment for follow-up with the specialist 4-6 weeks after your operation.
We will send a letter to your own doctor about your operation and the details of your treatment while you were in hospital.
Once Home
You should take regular pain relief as instructed by the nurse prior to your discharge. This helps to keep you comfortable so you are able to get about easier, do more and hence feel better.
Your wound should heal within a week. However, beneath your skin the muscle layers will take longer to heal. For this reason it is important to avoid any strenuous activity, heavy lifting and straining for 4-6 weeks. This includes things such as mowing lawns, gardening, vacuuming and lifting heavy washing baskets.
You can shower or bath at home, but you should not soak in the bath or use soap or powder directly on your wound until it has fully healed. You may need to place a dry dressing over your wound to collect any slight ooze so it does not stain your clothing or get dirty. It is important that your wound be kept clean and dry. Should you have any abdominal creases where your wound may remain moist, it is important to place a dressing between the creases to separate the skin and keep the area dry.
Avoid becoming constipated by keeping up a good fluid intake and eating fruit and foods high in fibre. If you have problems with constipation you may require a stool softener which you will be able to get from your nearest pharmacy.
Contact your own doctor if:
- Your wound becomes red, hot, swollen, and painful or continues to discharge.
- Your urine becomes cloudy, offensive smelling or you have any other signs of a urine infection.
- You have any concerns at all.
The important thing to remember is that you are not alone!
Nephrectomy is a relatively common operation and many people like you have undergone it with a high degree of success. Humans can survive easily on one kidney and there is no reason why you should not be able to function as you did prior to your surgery. A positive attitude on your part will make everything easier. There is every reason to believe that you will experience a successful outcome.
While you are in hospital, we will do everything we can to make your stay as comfortable as possible. The nursing and medical staff are always available to help with whatever needs you have. If you are worried about anything before or after your surgery, or if you have any further questions or would like more information, please do not hesitate to ask your nurse who will be more than happy to help.

