- Men
- Bilateral Scrotal Orchidectomy
- Bladder Neck Incision (B.N.I.) and Urethrotomy
- Brachytherapy
- Circumcision
- Cystoscopy
- Flexible Cystoscopy
- Hydrocelectomy Spermatocelectomy & Epididymal Cystectomy
- Inguinal Orchidectomy
- Kidney Cryotherapy
- Laparoscopic Nephrectomy
- Laproscopic Pyeloplasty
- Laser Prostatectomy
- Magnetic Resonance Imaging (MRI) Scan
- Nephrectomy
- Orchidopexy
- Other Services (Men & Women)
- Other Treatments (Men Only)
- Robotic Assisted Laparoscopic Prostatectomy
- Sexual Dysfunction
- Transperineal Ultrasound Guided Prostate Biopsy (TPPB)
- Transrectal Ultrasound & Biopsies of the Prostate
- Transurethral Resection of Bladder Tumour
- Ureteroscopy
- Vasectomy
- Women
- Children
- Clinical Trials
Treatment Process:
Ureteric Reimplantation
This information is designed to help you as parents understand your child’s condition and prepare for your child’s surgery. It will also help to plan how to take care of your child following discharge from hospital.
What is a Ureteric Reimplant and why is it needed?
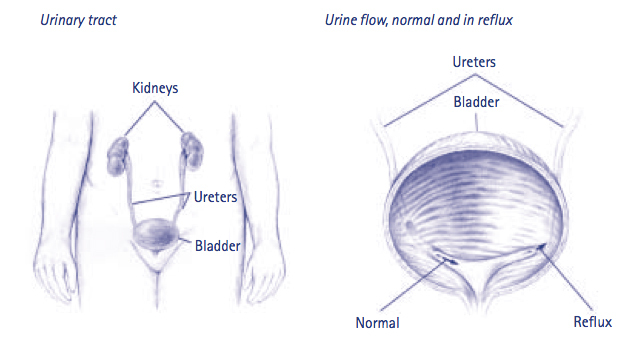
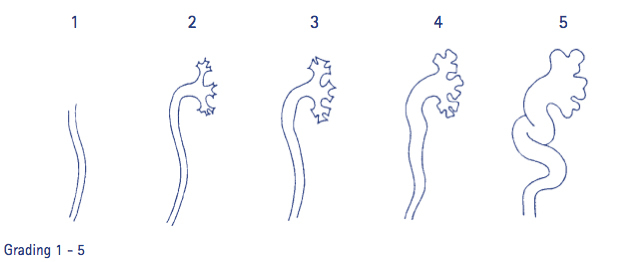
Your child has been diagnosed with vesico-ureteric reflux (“reflux”). This is a condition that allows urine to reflux (flow back up) the ureter to the kidney when the pressure in the bladder is increased. This is graded 1 – 5, with one being very minor and 5 being very severe. Grading is done on the basis of the findings at the cystogram, the x-ray procedure where dye is put into the bladder and observed entering the ureters and kidney. Children with reflux are susceptible to urine infections, which can lead to kidney scarring and damage or in more severe cases, the ureter and kidney becomes large, distorted and inefficient.
Treatment
A ureteric reimplantation is an operation to treat reflux. It may be one (unilateral) or both (bilateral) ureters that need repairing. Several factors can lead to surgical correction, including:
- The child does not tolerate antibiotics.
- Urine infections occur despite being on antibiotics.
- The reflux continues over several years of monitoring, i.e. the child does not “grow out of it”.
- The kidneys do not grow normally or start to develop scars on medical treatment alone.
- Parents request surgery as an alternative to medical treatment.
What does Ureteric Reimplantation involve?
The operation is done to correct the faulty “flap-valve” where the ureter enters the bladder and thus prevent reflux from occurring.
The child is anaesthetised and a small bikini line incision is made. Through this the bladder can be approached and opened. The opening of the ureter is found and a small circular incision is made around it. The ureter is dissected free from the bladder muscle. When the ureter can slide in and out of the bladder wall freely, a small tunnel is made for each ureter, approximately 2cm long, with the end opening into the bladder. The ureter is then passed through this tunnel and stitched into place. This is so that in the future, when the bladder muscle contracts to pass urine, the sides of the ureter will be pressed together and stop urine flowing back up to the kidney. The site of the original opening of the ureter is then closed and the bladder is also closed.
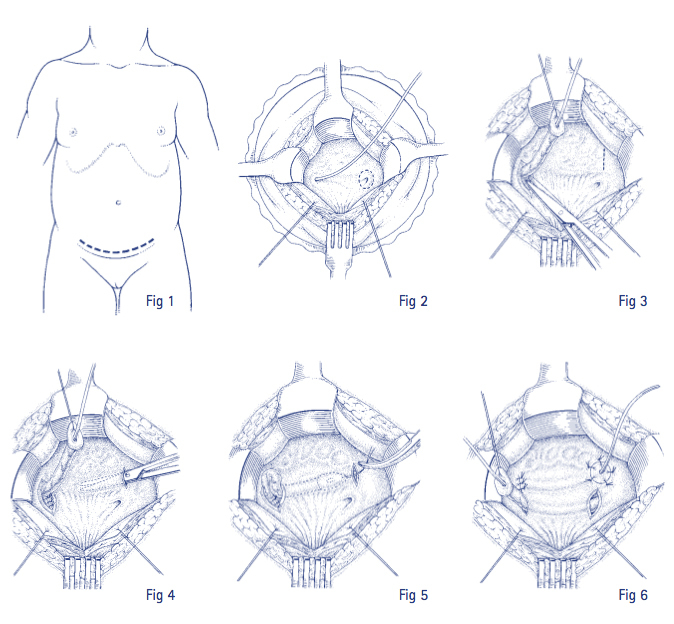
A catheter (flexible drainage tube) is left in the bladder and exits through the abdominal wound to drain urine out of the bladder to allow for healing to take place. Apart from the stitch holding the catheter in place, all other stitches are dissolving and will not need to be removed following the operation. A dressing is then placed over the wound and around the catheter to protect the incision and aid healing.
The operation can take anywhere from 1 – 3 hours, depending on whether one or both ureters are being reimplanted, and usually involves a 1 – 2 night stay in hospital, although some children can go home the same day.
What are the risks involved with surgery?
Complications such as wound or urine infection and bruising are uncommon. Because of the very high success rate and low risks involved with ureteric reimplant surgery, the operation is a very effective and safe way of treating reflux and preventing its long-term complications such as severe kidney damage. The chance of persistent reflux is very low, but failure is possible from not being adequately corrected. Ureteral stricture (narrowing) due to scarring is also rare. Approximately 5% of children who have had surgery on one side only for ureteric reflux then develop reflux on the other side, called ‘contralateral reflux’. This is monitored but usually disappears with time.
Your Consent
We need permission for the operation to go ahead. Before the consent is signed it is important that the risks and effects of the operation and anaesthetic are understood. These will be discussed prior to surgery. Should any questions arise after the discussion please feel free to ask the nurse or doctor who would be happy to answer these.
About Your Anaesthetic
Usually nothing is allowed to be eaten or drunk for six hours before surgery. This includes chewing gum and sweets. Exact instructions are given about ‘nil by mouth’ requirements prior to surgery. If the child does suck a sweet or take even a mouthful of food the operation will be postponed or even cancelled.
The operation is done under a General Anaesthetic. Patients are asleep throughout the operation and remember nothing of it. For young children gas is given through a small mask that puts the child off to sleep, and avoids the need for the insertion of a needle while the child is awake. However, as soon as the child is asleep, a drip is put in for safety reasons. A parent is encouraged to be present at the beginning of the anaesthetic. Once asleep a Caudal Block will be given. A needle is inserted into the back and medication is injected which makes the surgical area numb. This ensures the child will require less pain medication during the anaesthetic, and when they wake the caudal continues to work for several hours blocking the nerve supply to the operation site and preventing pain.
Feel free to ask the anaesthetist any questions.
Your Operation
On admission you will be informed of the approximate time of surgery and preparations will be completed by the nurse so your child is ready for theatre. Younger children are generally operated on before older children and where children are of similar age, shorter operations are done first.
You and your child will be escorted to the theatre waiting room. You and your child would then be taken to theatre and transferred to the operating table where anaesthetic staff will apply a mask and attach various monitoring devices. Once asleep you will be escorted from theatre and when all the preparations are complete and the anaesthetic has been given, surgery will begin.
When the operation is completed your child will go to the recovery room. You may be called up to recovery to meet your child. Your child will stay in the recovery room only for a short while where they will be cared for until they are ready to be transferred to the ward.
After Surgery
The nurse will check blood pressure, pulse and wound ooze routinely. A drip may be present to ensure adequate fluid intake is maintained until your child is drinking normally. They can usually eat and drink when they return to the ward. The catheter will drain the urine from the bladder into a bag. It is often blood stained for the first 48 hours.
Once recovered from the anaesthetic your child will be allowed to be up and about. However they may be a bit wobbly on their feet if they had a caudal anaesthetic so careful supervision will be needed. Pain relief is given on a regular basis to ensure comfort is maintained. At all times, the nurse is there to help, please ring the bell if assistance is needed and the nurse is not near by.
One parent is usually encouraged to stay overnight with your child. Please ask the ward on admission.
Going Home
Your child can go home once they are up and about, eating and drinking, and you feel happy about taking them home. This is usually the next day after surgery. A discharge information letter is given prior to going home and contains helpful information about caring for your child and their catheter when you return home.
The doctor will give a prescription for antibiotics after the operation to prevent a wound or urine infection. It is important to complete the whole course as instructed, even if all looks well.
You will be sent an outpatient appointment for follow-up 4 – 6 weeks after surgery. The doctor will then arrange for your child to have a check ultrasound scan of the kidney in 4 – 6 months time to ensure their is no blockage to the ureters and the kidneys are growing normally.
A letter is sent to your child’s own doctor about the operation and the details of treatment given in hospital. Failure is so rare that a follow up cystogram is no longer done routinely.
Once Home
It is important that your child avoids activities that may bump or pull on the catheter.
Regular pain relief can be taken as required to maintain comfort. Advice about pain relief will be given by the nurse prior to discharge. Prindette or Pamol syrup is usually prescribed for children and given every 4 – 6 hours.
Instructions about wound and dressing care will be given by the nurse prior to discharge. The dressing covering the wound should be peeled off on the fifth day like sticking plaster. Your child can shower or bath as usual.
The catheter bag needs to be emptied several times a day. The nurse will teach you how to care for the catheter prior to going home and give you sufficient supplies. Your child should be encouraged to drink plenty as this helps to prevent infection and flush out any bleeding. Urine may be passed urethrally as well as from the catheter. This is normal but can happen because of a kink or blockage in the tubing. For this reason, it is important to check the catheter regularly for any kinks and ensure it is positioned correctly. If your child is passing large amounts of urine urethrally and the catheter seems to be in order but there is no urine draining into the bag, it may mean the catheter is blocked and you need to contact the district nurse, the ward or your own doctor for advice.
A referral will be sent to the district nurse by the ward so they are available to visit or you can contact them should you have any problems or need advice with the wound or catheter care. They will usually call you before they visit if they have been instructed to take the catheter out. You will be instructed on how to clamp the catheter, usually on the fifth day once the bladder has had time to heal. Once your child has passed urine normally, the district nurse or the ward nurse can take the catheter out. Prior to having the catheter removed it helps to give your child a dose of Pamol or Prindette so they are more comfortable when the catheter is removed.
Many children have burning with urination and difficulty with bladder control as the bladder is healing. Passing blood in the urine is also expected. These symptoms generally resolve within 1 – 2 weeks, but can last longer in older children.
You should contact the ward or district nurse, or your own doctor for advice if your child is unwell or has any of the following:
- High temperature
- Not drinking or continually vomiting
- Excessive redness, swelling, discharge or bleeding around the wound or catheter
- Their urine becomes cloudy, smelly, heavily bloodstained or continues to sting
While your child is in hospital, we will do everything we can to make their stay as comfortable as possible. The nursing and medical staff are always available to help with whatever needs you have. If you are worried about anything before or after the surgery, or if you have any further questions or would like more information, please do not hesitate to ask the nurse who will be more than happy to help.

