- Men
- Bilateral Scrotal Orchidectomy
- Bladder Neck Incision (B.N.I.) and Urethrotomy
- Brachytherapy
- Circumcision
- Cystoscopy
- Flexible Cystoscopy
- Hydrocelectomy Spermatocelectomy & Epididymal Cystectomy
- Inguinal Orchidectomy
- Kidney Cryotherapy
- Laparoscopic Nephrectomy
- Laproscopic Pyeloplasty
- Laser Prostatectomy
- Magnetic Resonance Imaging (MRI) Scan
- Nephrectomy
- Orchidopexy
- Other Services (Men & Women)
- Other Treatments (Men Only)
- Robotic Assisted Laparoscopic Prostatectomy
- Sexual Dysfunction
- Transperineal Ultrasound Guided Prostate Biopsy (TPPB)
- Transrectal Ultrasound & Biopsies of the Prostate
- Transurethral Resection of Bladder Tumour
- Ureteroscopy
- Vasectomy
- Women
- Children
- Clinical Trials
Treatment Process:
Transurethral Resection of Bladder Tumour
This information is designed to help you, your family and friends prepare for your surgery. It will also help you plan how to take care of yourself in the weeks following discharge from hospital.
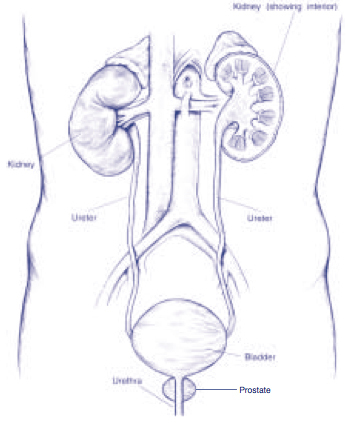
The bladder sits low within the pelvis and stores urine. It has two ureters that join to it from above, that transport urine from the kidneys. The urethra exits from the bottom of the bladder and through this, urine is passed to empty the bladder.
The Urologist has determined from the various tests you have had that it is likely that you have a bladder tumour and that surgical removal of the cancer is required.
Treatment
The operation is called a transurethral resection of bladder tumour (T.U.R.B.T.). This means that the tumour is removed through the urethra and no external incisions are needed. A special telescopic instrument called a resectoscope is passed into the bladder through the urethra using an anaesthetic lubricating gel.
A laser fiber or electric probe is then passed down the resectoscope and can be used to cut or burn the tumour from the inner layer of the bladder wall sealing off any bleeding areas at the same time. Any tissue that is removed is collected and sent to the laboratory where it is looked at under the microscope.
Many T.U.R.B.T’s are day stay procedures, which means that the majority of patients are able to return home on the same day as their operation.
Your Consent
We need your permission for your operation to go ahead.
Before you sign the consent form it is important that you understand the risks and effects of the operation and anaesthetic. Your doctor and the nurse will discuss these with you, should you have any questions, your nurse or doctor would be happy to answer these.
It would be a very rare occurrence to require a blood transfusion with this surgery. However, in the unusual event that you did need a blood transfusion and you want to refuse one, it is vital that you tell your surgeon and nurse prior to your operation.
About Your Anaesthetic
You will NOT be allowed to eat or drink anything for at least six hours before your surgery. This includes chewing gum and sweets.
There are two main types of anaesthetic used for this surgery;
- General Anaesthetic: You will be asleep throughout the operation and remember nothing of it.
- Regional Anaesthetic e.g. Spinal, Epidural or Caudal: A needle is placed into your back and a solution is injected that will numb your body from the waist down. You will be awake but maybe sleepy and you will not feel the operation.
Feel free to discuss these options, and your questions with the anaesthetist.
You must not drive any vehicle or operate any machinery for 24 hours after having an anaesthetic. You will have to arrange for someone to drive you home if you go home within 24 hours of your surgery.
Your Operation
On admission, you will be informed of your approximate time of surgery and prepared for theatre by your nurse.
You may be given some tablets before theatre. These are charted by your anaesthetist and may include tablets for tension, nausea and pain prevention.
You will be escorted to the theatre, where you will be transferred to the theatre table. Anaesthetic staff will then insert a drip in your arm and attach various monitoring devices.
Once you have been completely prepared and given your anaesthetic, surgery will begin. The operation can take anywhere from 15 minutes to an hour depending on the size and number of tumours involved.
When the operation is completed, you will go to the recovery room for a short while where you will be cared for until you are ready to be transferred to the ward.
After Surgery
Your nurse will check your blood pressure, pulse and temperature routinely.
Dependent on how long the surgery takes and how much bleeding there is you may or may not have the following after surgery:
- A drip to keep you well hydrated after your surgery. This will be removed once you are drinking normally. You can usually eat and drink when you return to the ward.
- A catheter (drainage tube that passes through the urethra into the bladder) to drain the urine into a bag. The catheter is held in place inside the bladder by a small balloon so that it cannot slip out. The catheter is normally removed the following morning after surgery but in some instances, it may even be removed when you return to the ward from the recovery unit. When the catheter is removed, the balloon is deflated by using a special device located at the end of the catheter where it connects to the drainage bag. The catheter slides out easily once the balloon is deflated causing little discomfort. If you do not have a catheter or once your catheter is removed, you will be asked to pass your urine into a urine bottle or pan so it can be measured and the amount of blood in the urine can be assessed. Your urine is likely to be blood stained after surgery but this usually clears within the first 48 hours.
- Continuous bladder irrigation which is fluid that runs by gravity into the bladder and out again through the catheter. Bladder irrigation is used only if necessary to help stop any ongoing bleeding. This is usually removed the morning following your surgery and the catheter is removed later that day or the following morning.
After surgery you may or may not experience some of the following symptoms:
- A burning sensation and the desire to go to the toilet. These symptoms are not usually caused by a full bladder but by the irritation caused by the removal of the bladder tissue. These symptoms are easily treated with mild pain relievers and medications which change the acidity of the urine.
- A stinging or burning sensation, either when passing urine, or at the tip of the penis in males or within the urethra in females. This is usually due to the urine, which is naturally acidic, coming into contact with any raw areas in the urethra or it can be caused by the instruments used during the operation. These symptoms are easily relieved with medication or the application of an anaesthetic gel for males.
- A feeling of having a full bladder if you have a catheter in. This can be caused by blockage of the catheter tube either by a blood clot or by an accidental kink of the tube. These blockages are easily cleared by the nurse.
- Bladder spasms, due to the bladder trying to expel the catheter or because of bladder irritation. These are once again easily treated with medication.
Our aim is to keep you as comfortable as possible, it is important that the nurse know when the pain or discomfort starts so your symptoms can be relieved as quickly and easily as possible. At all times, your nurse is there to help you, please ring your bell if you need assistance and your nurse is not nearby.
Once you have recovered from the anaesthetic your nurse will help you, to get out of bed for the first time. If you have had a spinal anaesthetic, you may be asked to lie flat for several hours after returning to the ward to allow for the anaesthetic to wear off.
You will be asked to drink extra fluids after your surgery and for the next few weeks after your discharge. This helps flush the bladder, which clears up bleeding, washes away debris and helps prevent infection. You should drink approximately 1500mls, which is about eight glasses of fluid per day. Water is best but any fluid is O.K. There is no need to drink excessive amounts of fluid; once the urine is free of blood you should drink just enough to keep your urine a pale yellow to clear colour.
Going Home
Once you are catheter free, eating and drinking and you have passed urine you will be able to return home. This is either the same day as your operation or maybe the following day.
Before leaving the ward you will be given a discharge information letter which contains helpful information for when you get home.
Depending on your individual case, follow-up will be arranged which may either involve an outpatient visit 4-6 weeks after surgery, or a flexible cystoscopy in 3-6 months. You will be informed of the expected follow-up, which may continue for many years after your surgery. Close monitoring after having a T.U.R.B.T is very important to diagnose any cancer recurrence so that treatment can be given to keep things well under control.
You may be given a prescription for medication to take only if specifically requested by the doctor. If you are prescribed antibiotics to take it is very important that you complete the whole course of tablets, even if you feel better and don’t think they need to be finished.
We will send a letter to your own doctor about your operation and the details of your treatment while you were in hospital.
Once Home
It takes time for the raw surface inside the bladder to heal. Until it does you may experience a burning sensation when passing urine, urgency (the need to void in a hurry), and frequency (the need to void often). These symptoms subside as healing progresses and can be relieved with the help of powders to neutralise the urine and other medication such as mild pain relievers that your nurse will inform you about. Should these symptoms continue for longer than a few days and if they are at all associated with cloudy, offensive smelling urine you should contact you own doctor as soon as possible as these signs are indicators of a urine infection.
You may notice that you pass a little blood when going to the toilet, this is usually at the beginning of the urine stream. This is normal after this surgery and nothing to be concerned about. The urine may clear totally between times but for up to 4 weeks after your surgery you may get slight bleeding. This is the normal process of healing and you need only be concerned if you have fresh heavy bleeding that does not stop or if your are unable to pass your urine at all which may be due to a blood clot blocking the urethra. If either of these unlikely events should occur you should contact your own doctor immediately or go to your nearest emergency department.
Continue to drink plenty of fluid if bleeding persists, otherwise drink enough to keep your urine a pale yellow to clear colour.
You can get back to most activities except for any heavy lifting, straining or strenuous activity which should be avoided for 4-6 weeks after your surgery. This includes things such as any digging in the garden, mowing the lawns, vacuuming and lifting heavy baskets of washing as these activities can cause renewed bleeding. Apart from these strenuous activities, you will be able to continue with your normal daily routines as you feel able.
Before discharge, your nurse will inform you about taking mild pain relievers, should you have any pain or discomfort after you return home.
Depending on the size of tumour this is routinely a straightforward operation, after which most patients have a very speedy recovery.
While you are in hospital, we will do everything we can to make your stay as comfortable as possible. The nursing and medical staff are always available to help with whatever needs you have. If you are worried about anything before or after your surgery, or if you have any further questions or would like more information, please do not hesitate to ask your nurse who will be more than happy to help.

